Introduction
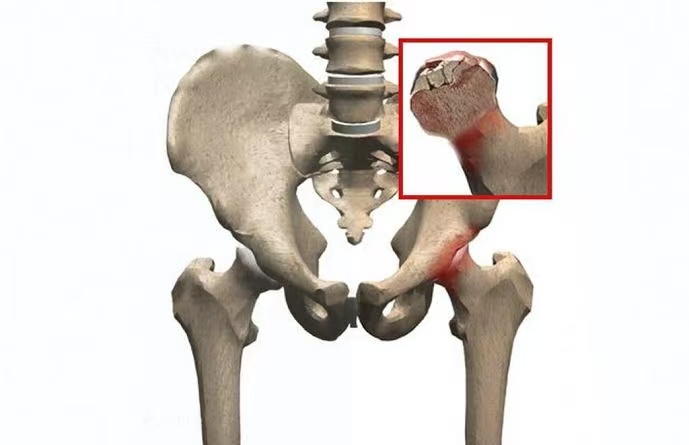
Avascular necrosis (AVN), also known as osteonecrosis, is a pathological condition characterized by the death of bone tissue due to a lack of blood supply. When AVN affects the femoral head—the ball-shaped upper end of the thigh bone (femur) that fits into the hip socket—it can lead to the collapse of the bone structure, resulting in joint dysfunction and severe arthritis. This condition predominantly affects individuals between the ages of 20 and 50 and can significantly impair mobility and quality of life.
Pathophysiology
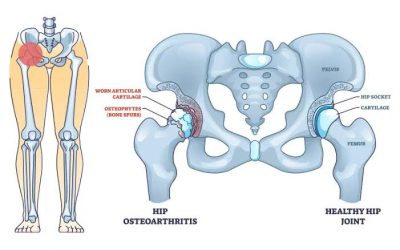
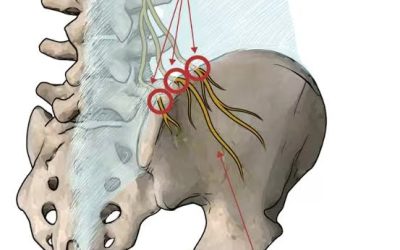
The femoral head relies on a delicate network of blood vessels for nourishment. Disruption of this blood supply, whether due to trauma or other factors, leads to ischemia and subsequent death of bone cells (osteocytes). As the bone tissue deteriorates, the structural integrity of the femoral head is compromised, potentially leading to its collapse. This collapse can cause the articular cartilage covering the bone to deteriorate, resulting in joint pain and osteoarthritis.
Causes and Risk Factors
Traumatic Causes
Trauma is a common cause of AVN of the femoral head. Injuries such as hip dislocations or fractures can damage the blood vessels supplying the femoral head, leading to ischemia. For instance, osteonecrosis is observed in 10–25% of hip dislocations, with increased risk associated with prolonged duration of dislocation. The incidence of traumatic AVN following nondisplaced femoral neck fractures is approximately 10%, whereas the incidence following displaced fractures ranges from 15% to 50% and generally correlates with the degree of displacement, time until reduction, and accuracy of reduction.
Non-Traumatic Causes
Non-traumatic AVN is often associated with various risk factors:
- Corticosteroid Use: Prolonged use of corticosteroids is a significant risk factor. These medications can interfere with the body’s ability to break down fatty substances, leading to blockages in blood vessels.
- Alcohol Consumption: Excessive alcohol intake can cause fatty deposits in blood vessels, reducing blood flow to bones.
- Medical Conditions: Diseases such as sickle cell anemia, lupus, and Gaucher’s disease can compromise blood flow.
- Radiation Therapy and Chemotherapy: These treatments can damage blood vessels and bone tissue.
- Blood Clotting Disorders: Conditions that increase blood clotting can obstruct blood flow to the femoral head.
- Other Factors: Smoking, pancreatitis, chronic liver disease, and HIV infection have also been linked to AVN.
In some cases, the exact cause remains idiopathic, meaning it is unknown.
Symptoms
AVN of the femoral head often progresses silently in its early stages. As the condition advances, symptoms become more apparent:
- Pain: Initially, patients may experience mild discomfort in the groin, thigh, or buttock. As the disease progresses, the pain intensifies, especially during weight-bearing activities.
- Limited Range of Motion: Stiffness and decreased mobility in the hip joint are common.
- Limping: To alleviate pain, individuals may develop a limp or favor the unaffected leg.
- Progression to Osteoarthritis: Without intervention, the joint may deteriorate, leading to osteoarthritis.
Diagnosis
Early diagnosis is crucial for effective management. The diagnostic process includes:
- Medical History and Physical Examination: Assessing risk factors and evaluating hip function.
- Imaging Studies:
- X-rays: May appear normal in early stages but can reveal bone collapse in advanced stages.
- MRI: Highly sensitive in detecting early bone changes before they appear on X-rays.
- CT Scans: Provide detailed images of bone structure.
- Bone Scans: Can detect changes in bone metabolism.
- Biopsy: Rarely performed but can confirm the diagnosis.
Treatment Options
Treatment aims to preserve the femoral head, alleviate pain, and restore function. Approaches vary based on the stage of the disease:
Non-Surgical Treatments
Effective in early stages before bone collapse:
- Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) to manage pain.
- Reduced Weight Bearing: Using crutches or limiting activities to decrease stress on the hip.
- Physical Therapy: Exercises to maintain joint mobility and strength.
- Bisphosphonates: Drugs that may slow bone damage.
- Hyperbaric Oxygen Therapy: May promote healing by increasing oxygen supply to the bone.
Surgical Treatments
Considered when non-surgical methods are ineffective or in advanced stages:
- Core Decompression: Removing a portion of the inner bone to reduce pressure and stimulate blood flow.
- Bone Grafting: Transplanting healthy bone tissue to support the femoral head.
- Osteotomy: Reshaping the bone to redistribute weight and relieve stress on the affected area.
- Total Hip Replacement: Replacing the damaged hip joint with an artificial one, typically used in advanced cases.
- Regenerative Medicine: Emerging treatments involving stem cells to promote bone regeneration.
Prognosis
The outcome depends on the stage at diagnosis and the effectiveness of treatment:
- Early Detection: Increases the likelihood of preserving the femoral head and preventing joint collapse.
- Advanced Stages: Often require surgical intervention, with total hip replacement being common.
Regular follow-ups and adherence to treatment plans are essential for optimal outcomes.
Conclusion
Avascular necrosis of the femoral head is a serious condition that can lead to significant disability if not addressed promptly. Understanding the risk factors, recognizing early symptoms, and seeking timely medical intervention are crucial steps in managing the disease. Advancements in both surgical and non-surgical treatments offer hope for preserving joint function and improving the quality of life for affected individuals.